

Last month I arrived in Nuuk ready to start up our project of examining the Inuit diet.
As you can read in an earlier blog post, we are examining the effect of this diet and how it could potentially be used to prevent the rising type 2 diabetes prevalence among the Greenland Inuit population.
Setting up a trial is always a bit chaotic and stressful since a lot of unknowns needs to come together. We started by sending a bunch of letters to potential participants. This was done manually, so Else, our Greenlandic project employee (it’s hard to find a good name for her position – basically she is essential in all parts of the project from examinations, recruitment to the handling of everyday project related activities) had her work cut out for her.
Next up we went buying foods for the participants. We have a deal with one of the local supermarkets, Brugseni, which has a large selection of both Danish and Inuit foods and who helps us with handing out the foods. Since we did not have enough freezer storage at our examination site this was a huge help leaving one of the logistic unknowns solved. We ended up providing the participants with a wide range of foods. For the traditional Inuit diet, this included a selection of fish (cod, halibut, salmon, trout, etc.), seafood (shrimps) and sea mammals (whale, seal). For the westernized diet we provided a 28-day box with frozen imported meats (incl. beef, lamb, pig, sausages, chicken and cold cuts of meat), various pasta, cereals, and bread (both rye bread and white bread). We went for providing foods for the participants covering around 25% of their daily energy intake and thus the participants need to cover some of the foods themselves. They got a detailed pamphlet on which foods to consume and which foods to avoid when being on the different diets. Luckily the participants were very enthusiastic about the study, especially the traditional Inuit diet.


One of the traditional ways of living in a hunter-gatherer society is collecting your own food. Fishing is still a big part of society in Greenland and for the period where the participants are encouraged to eat an Inuit diet, they are encouraged to eat locally caught fish. I got to try this out while being on a local boating trip, where our guide asked whether we would like to try to fish. In Denmark, this can be a lengthy process taking hours with very little success. However, our guide assured us that we would, of course, catch something; it would take a maximum of 30 min. I was skeptical, but went along with it, even though I have only tried fishing once or twice. To my amazement, I was able to pick up 8 sizeable codfish and another tourist from the boat trip picked up 9 codfish – all in 30 min. Here you see a picture of me getting it ready for consumption – an amazing dinner – really showing the amazing tastes of the Greenland Inuit cuisine.
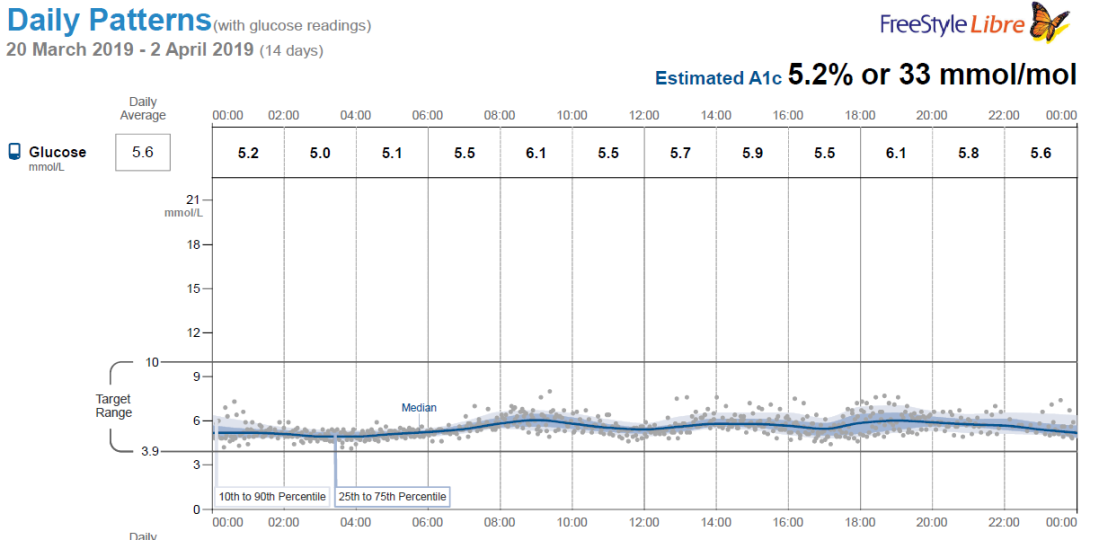
Of course, we also need to examine the participants and a special focus for this trial is to test how the diet affects the blood sugar regulation in order to understand whether it can ultimately prevent the participants from developing type 2 diabetes. We do this in multiple ways. First, we examine the participant’s blood sugar when they arrive at the examinations, also called fasting blood sugar. If this is elevated you will have a higher risk of developing type 2 diabetes. Furthermore, we examine their HbA1c or glycated hemoglobin. This is a marker of longer-term average blood glucose levels (8-12 weeks). Hemoglobin is normally what carries oxygen in the blood, however, when hemoglobin is exposed to glucose in the blood, it can also bind glucose and we can measure if the hemoglobin has been exposed to higher levels of glucose over the preceding weeks. To further test how well the participants handle their blood glucose we also do an oral glucose tolerance test. In this test, the participants consume 75 gram of glucose in 150 ml of water within 5 min (yes it’s very sweet!) and then we measure their blood sugar over the next two hours. This tells us something about how well they can handle a large amount of sugar – the better they can do this (with lower blood sugar) the lower the risk of developing type 2 diabetes. One last way we assess their blood sugar regulation in this study is providing the participants with a small glucose monitor, which we place on their upper arm. This can measure their blood sugar continuously for 14 days in a row (!) and provide very detailed data on how their blood sugar is behaving during the two diet periods. Below you can see an example of how it looks when we have measured the blood sugar for 14 days. We hope that this can make us much more knowledgeable about how we can use the diet to regulate blood sugar, something which can be both of importance when preventing but also treating type 2 diabetes. Besides looking into the blood sugar regulation of the participants, we also examine various other markers in their blood such as their cholesterol level and level of inflammation, but that will be a story for another time.
For now, the study is up and running and we are looking forward to seeing the first results. However, there is still a lot of work to do and we need to plan for the next two study sites in Qaanaaq (the northwest of Greenland) and in Qasigiannguit in the Disco Bay (west Greenland). Hope you enjoyed the update on the Greenland Inuit diet project and I look forward to writing the next update on the project.




 I’m happy to announce that I’m working on a new project which is centered around a dietary intervention study in Greenland. The overall objective of the study is to investigate a traditional Inuit diet compared to a westernized diet in Greenland Inuit. The reason we are examining this is that the lifestyle of Inuit in Greenland is undergoing a transition from a fisher-hunter society, with a physically active lifestyle and a diet based on the food available from the natural environment, to a westernized society. Parallel to this, a rapid increase in the prevalence of lifestyle diseases such as type 2 diabetes and obesity has been observed[1]. What we are especially interested in is whether switching to a more traditional Inuit diet could improve glycemic control and thus prevent the development of type 2 diabetes.
I’m happy to announce that I’m working on a new project which is centered around a dietary intervention study in Greenland. The overall objective of the study is to investigate a traditional Inuit diet compared to a westernized diet in Greenland Inuit. The reason we are examining this is that the lifestyle of Inuit in Greenland is undergoing a transition from a fisher-hunter society, with a physically active lifestyle and a diet based on the food available from the natural environment, to a westernized society. Parallel to this, a rapid increase in the prevalence of lifestyle diseases such as type 2 diabetes and obesity has been observed[1]. What we are especially interested in is whether switching to a more traditional Inuit diet could improve glycemic control and thus prevent the development of type 2 diabetes.

